Gustafsson S, Sehlin D, Lampa E, et al. "Heterogeneous drug tissue binding in brain regions of rats, Alzheimer's patients and controls: impact on translational drug development." Sci Rep. 2019;9:5308. https://doi.org/10.1038/s41598-019-41828-4
Background
Understanding regional drug tissue binding in the brain is critical for CNS drug development. Gustafsson et al. (2019) asked a straightforward question: is drug tissue binding uniform across different brain regions in rats, Alzheimer's disease (AD) patients, and age-matched controls?
Methods
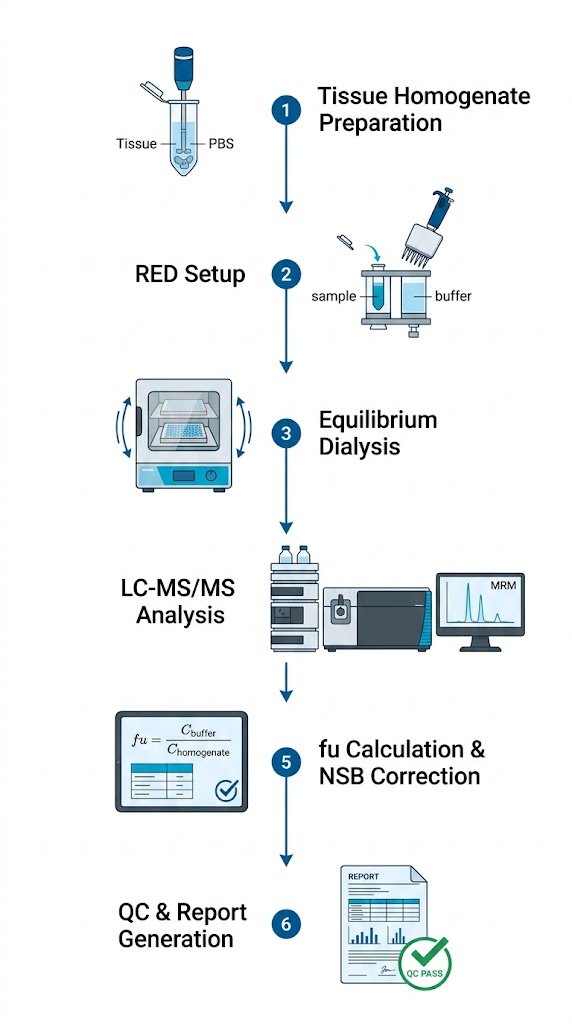
The team used equilibrium dialysis combined with LC-MS/MS to measure fu,brain,ROI for three CNS drugs — citalopram, donepezil, and risperidone — across five brain regions (frontal cortex, temporal cortex, hippocampus, thalamus, and striatum). Brain tissue homogenates were prepared at a 1:4 dilution in PBS, dialyzed against buffer for 5 hours at 37°C, and analyzed by LC-MS/MS.
Results
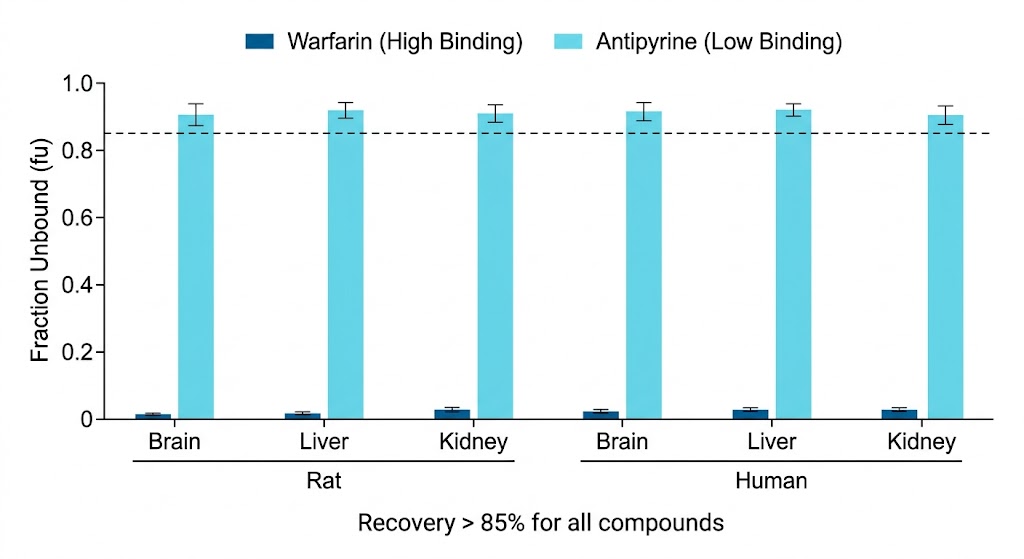
The answer was no — regional binding is far from uniform. Donepezil showed a 2.5-fold difference in fu between the hippocampus (fu = 0.038) and the thalamus (fu = 0.095) in human AD brain tissue. Regional binding patterns also differed between AD patients and controls, suggesting that disease state alters tissue composition and binding characteristics. In rats, the variability was less pronounced but still present, with the lowest fu values consistently in the hippocampus.
Conclusions
Single-region brain tissue binding measurements may not adequately represent the entire brain for CNS drug development. Multi-region assessment — an approach we routinely offer — provides more accurate Kp,uu,brain values and improves PBPK model predictions for CNS-active compounds.