Why RAAS Cascade Evaluation Often Fails in Cardiorenal Studies
Single-analyte RAAS measurements often mislead cardiorenal studies. Vasoactive peptides degrade rapidly after collection, and highly homologous angiotensin metabolites are notoriously difficult to distinguish using standard immunoassays.
| Analytical Problem | Why It Happens | Impact on R&D Decisions |
|---|---|---|
| Rapid Ex Vivo Degradation | Vasoactive half-lives are extremely short (seconds to minutes); endogenous proteases continue cleaving post-collection. | Physiological baselines are artificially lost, masking true pharmacological responses and target engagement. |
| Sequence Homology | Angiotensin II, III, and 1-7 differ by only 1-2 amino acids, presenting structural challenges for antibodies. | ELISA cross-reactivity can cause false-positive signals, misguiding mechanism-of-action interpretations. |
| Fragmented Data | Standard assays measure isolated targets rather than capturing the complete precursor-to-product pathway. | It becomes impossible to accurately calculate critical in vivo enzymatic shifts (e.g., ACE vs. ACE2 balance). |
How This Panel Supports Cardiorenal Pharmacodynamics
To make confident go/no-go decisions, researchers must evaluate the dynamic balance of the endocrine system. Our panel translates absolute quantification into actionable mechanistic insights.
What This Panel Helps You Decide:

Confirm Target Engagement
Prove whether your novel modulators effectively block or stimulate specific cascade nodes in vivo.

Classic vs. Alternative RAAS
Track the shift from vasoconstrictive/profibrotic pathways (Ang II) to cardioprotective pathways (Ang 1-7).

Circulating vs. Local RAAS
Determine if efficacy is driven by systemic blood pressure lowering or specific local tissue receptor blockade.

Interpret Endothelial Remodeling
Utilize ultra-low abundance ET-1 and Bradykinin levels to assess vascular tone and endothelial health.
How We Address Peptide Instability and Sequence Homology
We secure robust data through two foundational pillars: absolute sequence-specific mass spectrometry and rigorous pre-analytical stabilization protocols.
A. Sequence-Level Specificity
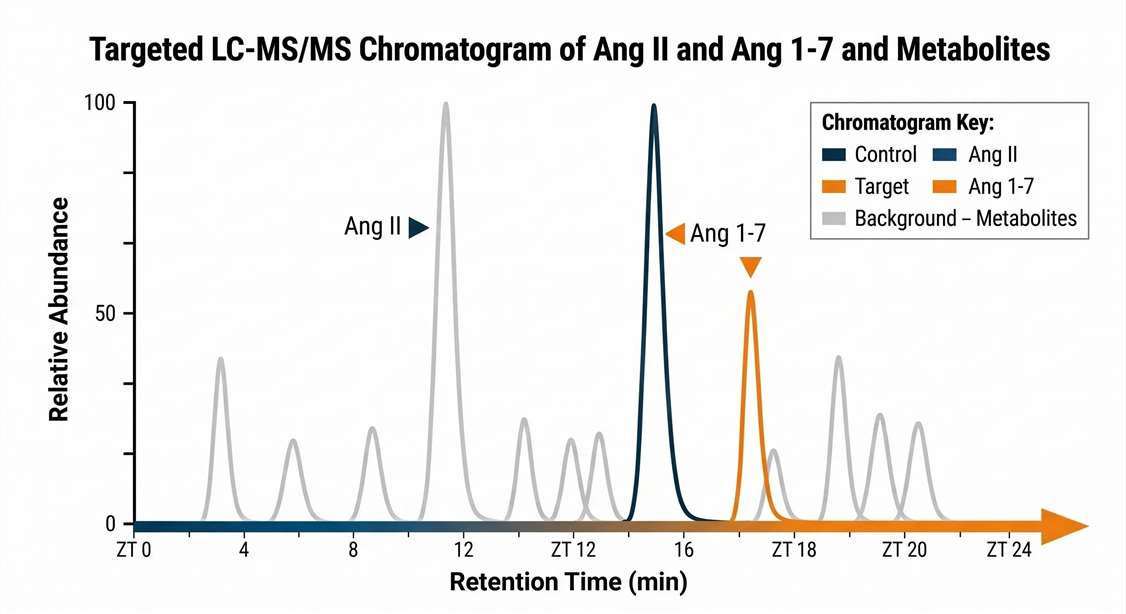
- Targeted LC-MS/MS distinctly separates isobaric and highly homologous peptides based on exact mass-to-charge (m/z) ratios and specific fragmentation patterns.
- Significantly mitigates the cross-reactivity risks inherent to traditional antibody-based kits.
- Allows for the simultaneous, unbiased quantification of precursors, active products, and inactive metabolites.
B. Stabilization Strategy
Standard Collection (High Risk)
Relying on standard EDTA alone fails to inhibit neprilysin or aminopeptidases, resulting in rapid peptide cleavage and a complete loss of the physiological baseline.
Targeted Stabilization (Our Standard)
We deploy proprietary, multi-target protease inhibitor cocktails precisely at the moment of collection to arrest enzymatic activity and freeze the in vivo profile.
Configurable RAAS Panel: Classic, Alternative, and Endothelial Pathways
Depending on your therapeutic target, our panel can be configured to cover essential functional domains of blood pressure regulation and vascular tone.
| Functional Axis | Selected Target Analytes | Relevance to Drug Discovery |
|---|---|---|
| Classic RAAS Axis | Angiotensin I, Angiotensin II, Angiotensin III, Aldosterone | Systemic vasoconstriction and profibrotic signaling. Critical for ARBs and ACE inhibitors. |
| Alternative RAAS Axis | Angiotensin 1-7, Angiotensin 1-9, Angiotensin IV | Vasodilation and anti-hypertrophic effects. Essential for assessing ACE2 modulators. |
| Vascular Tone & Endothelial | Bradykinin, Endothelin-1 (ET-1), Substance P | Modulators of local vascular resistance. Important for pulmonary hypertension models. |
| Volume Regulation | Atrial Natriuretic Peptide (ANP), Brain Natriuretic Peptide (BNP) | Preclinical indicators of ventricular stretch and heart failure progression. |
This panel integrates seamlessly with targeted proteomics for cardiac injury markers and targeted lipidomics for eicosanoid profiling to provide a holistic view of cardiopulmonary health.
Pre-Analytical Stabilization: Conditions for Project Success
Standard plasma collection is insufficient. To prevent baseline failure, the integrity of your bioanalytical data strictly depends on these pre-analytical execution conditions:
Immediate Inhibitor Exposure
Strict Cold-Chain Handling
Snap-Freezing for Local RAAS
Matrix-Specific Homogenization
1
Immediate Inhibitor Exposure
Blood must be drawn directly into pre-chilled tubes containing specialized, multi-target protease cocktails to instantly block degradation pathways.
2
Strict Cold-Chain Handling
Samples must be processed and centrifuged at 4°C within minutes of collection to suppress any residual enzymatic cleavage effectively.
3
Snap-Freezing for Local RAAS
Tissues intended for local RAAS analysis must be excised and flash-frozen in liquid nitrogen (< 30 seconds) to completely halt local tissue proteases.
4
Matrix-Specific Homogenization
Temperature-controlled extraction buffers tailored to overcome the dense lipid and protein barriers unique to heart and kidney tissues.
Applications in Hypertension, Heart Failure, and Renal Disease
Our targeted analytical workflows are designed to support precise R&D tasks across preclinical and clinical pharmacology:
Representative Deliverables and Decision Outputs
We deliver structured, context-rich data designed to directly answer your mechanistic and pharmacological questions.
ACE / ACE2 Surrogate Ratio Analysis
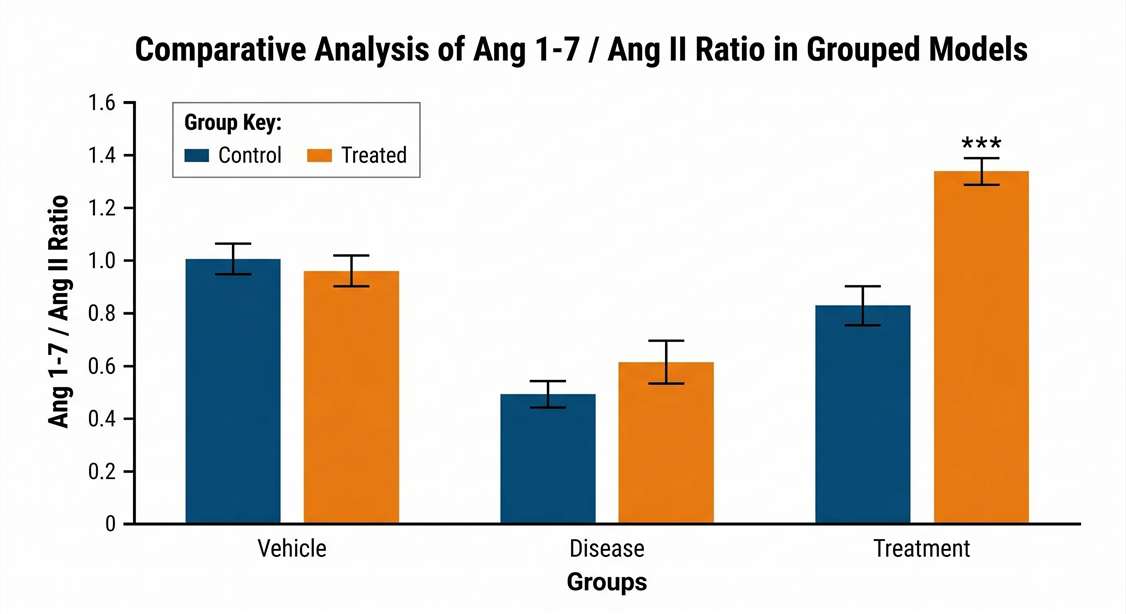
Calculate Ang II/Ang I or Ang 1-7/Ang II ratios to accurately estimate in vivo enzymatic shifts and pathway balance.
Drug-Response Group Stratification
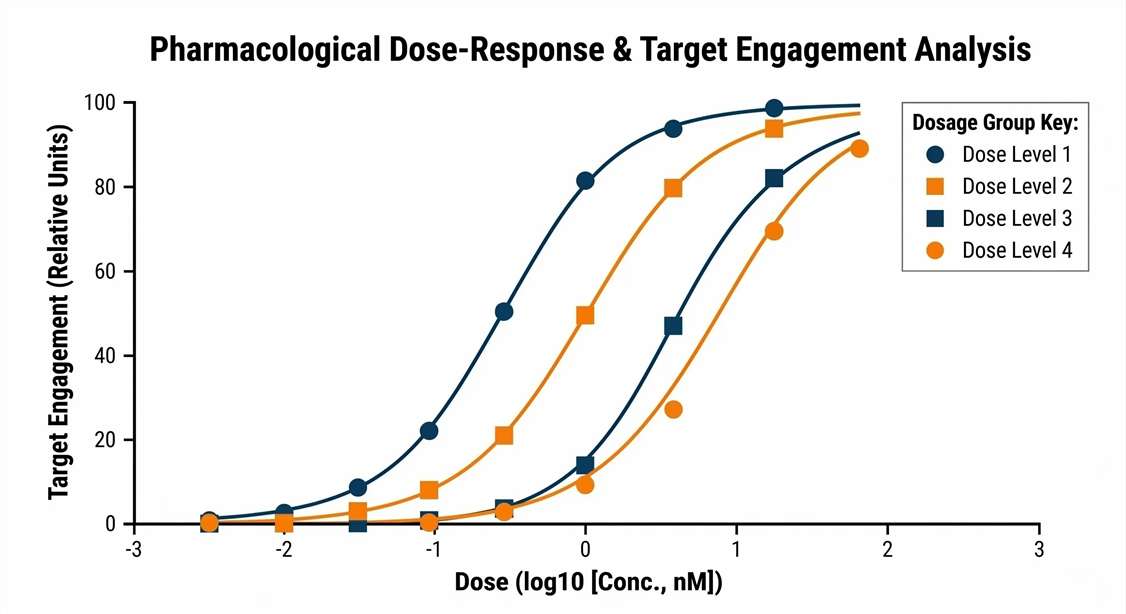
Utilize overlay plots to confirm how different doses of your candidate compound rebalance the neuroendocrine cascade.
Local vs. Systemic RAAS Comparison
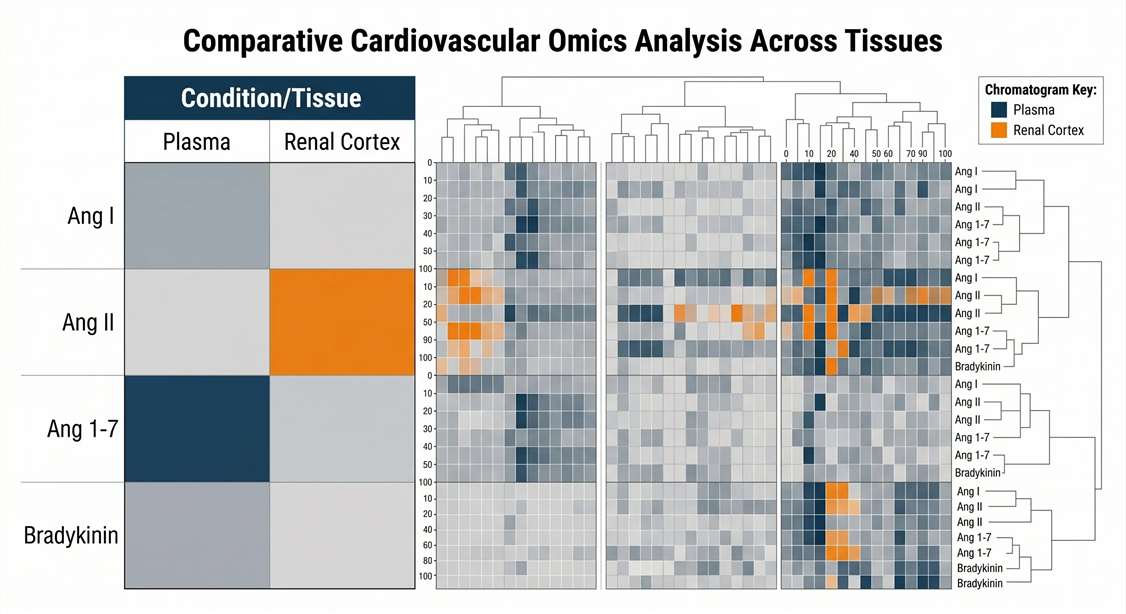
Match plasma and tissue data to prove target-organ specific penetration, evaluating if efficacy is driven centrally or peripherally.
Bioanalytical QC Package
Receive comprehensive validation metrics including LLOQ and complex matrix recovery rates for ultimate IND-ready data confidence.
Sample Requirements Aligned with Target Stability
To ensure the integrity of the target analytes, specific stabilization matrices are mandatory.
| Matrix Type | Species / Context | Min Volume / Mass | Critical Pre-Analytical SOPs |
|---|---|---|---|
| Blood (Plasma) | Rodent, NHP, Human | 100 μL | Standard EDTA is insufficient. Must be collected into pre-chilled tubes containing specific inhibitor cocktails tailored to target peptides. |
| Tissue (Kidney/Heart) | Rodent Models | 30 - 50 mg | Tissue must be snap-frozen in liquid nitrogen immediately (< 30 seconds) upon excision to halt local tissue proteases. |
| Cell Supernatant | Ex vivo / In vitro | 200 μL | Protease inhibitor cocktails must be added immediately upon collection, followed by prompt freezing. |
(Consult with our scientific team prior to initiating your in vivo study. We provide tailored guidance on stabilization protocols and custom targeted mass spectrometry quantitation of neuropeptidomics workflows.)
Frequently Asked Questions (FAQ)
Why is targeted LC-MS/MS preferred over ELISA for the Angiotensin family? +
Immunoassays are highly cost-effective for screening isolated targets. However, members of the Angiotensin family differ by only a single amino acid cleavage. This homology increases the risk of antibody cross-reactivity. Targeted LC-MS/MS differentiates these molecules based on exact molecular mass and distinct fragmentation patterns, helping to confidently separate active targets from inactive metabolites.
Can you measure local RAAS activity in kidney or heart tissue? +
Yes. While systemic RAAS provides valuable information, local tissue RAAS is often a stronger driver of target-organ fibrosis. We utilize specialized extraction techniques designed to overcome the dense lipid and protein matrices of the heart and kidney, allowing for the precise quantification of locally generated vasoactive peptides.
Why do I need a specialized protease inhibitor cocktail instead of just EDTA? +
EDTA primarily inhibits metalloproteases by chelating divalent cations. However, the degradation of vasoactive peptides is driven by a diverse array of enzymes, including aminopeptidases, neprilysin, and chymases, which are not fully inhibited by EDTA alone. A multi-target cocktail is required to thoroughly suppress ex vivo enzymatic activity and preserve the in vivo baseline.
How do RAAS peptide ratios reflect in vivo enzyme activity? +
The concentration of a product relative to its precursor serves as a practical indicator of the enzyme mediating that conversion. For instance, an increase in Angiotensin I coupled with a decrease in Angiotensin II suggests an inhibition of ACE. Utilizing these ratios helps to normalize baseline individual variations and provides a clearer picture of pathway-specific drug effects.
Disclaimer: All services and analytical platforms described are intended for translational research and preclinical support. Research Use Only (RUO). Not for use in diagnostic procedures.