
Liquid biopsy research is no longer just a race to detect something tumor-derived in blood. For pancreatic, lung, and breast cancer programs, the practical challenge is to detect actionable biology early, separate malignant from inflammatory noise, and then verify candidate markers at scale with workflows that are reproducible across cohorts.
This article is optimized for researchers evaluating exosome liquid biopsy protein biomarkers and building verification-ready multi-protein panels.
Among the major analytes used in preclinical and translational settings—circulating tumor DNA (ctDNA), circulating tumor cells (CTCs), and extracellular vesicles (EVs)—tumor-derived exosomes are increasingly treated as a uniquely information-rich compartment. They are shed continuously, protect their cargo from enzymatic degradation, and can carry surface and luminal proteins that reflect tumor state, immune interactions, and metastatic potential.
This resource focuses on exosomal protein biomarker signatures (not single markers) and how they are being used in preclinical studies of pancreatic ductal adenocarcinoma (PDAC), lung cancer, and breast cancer. The throughline is a shift in experimental strategy: from "find a marker" to "build a classifier," and from small discovery cohorts to targeted, high-throughput verification.
The Proteomic Shift in Liquid Biopsy Research: How Exosomes Complement ctDNA
ctDNA and CTCs remain foundational in oncology liquid biopsy research, but both face structural constraints that are especially punishing in early-stage or localized tumor models.
ctDNA detection can be biologically constrained at low tumor burden. In stage I disease models (and in many early-stage clinical cohorts used for translational benchmarking), the fractional abundance of tumor-derived DNA fragments can fall below practical detection thresholds. Even with improved error suppression and deeper sequencing, the core issue remains: if shedding into circulation is sparse, there is simply not enough signal to recover.
CTCs are information-dense but statistically rare. CTC-based studies can be powerful for phenotyping and functional work, but many cohorts yield very low counts per tube of blood. That scarcity drives sampling noise, increases the risk of false negatives, and complicates longitudinal study designs where the question is "did the marker change?" rather than "is anything there?"
Tumor-derived exosomes (often discussed as TEX) offer a different experimental advantage: they are active biological broadcasters. Exosome secretion is not a passive leak; it is a regulated process linked to stress responses, immune modulation, and microenvironment remodeling. Because exosomes are shed into circulation even when the primary tumor is small, they can provide earlier access to tumor-associated biology than analytes that require higher tumor burden to become measurable.
From a proteomics perspective, exosomes also behave like natural "enrichment containers." Their lipid bilayer protects proteins from proteases and reduces the impact of short-term handling variability relative to free proteins. For translational teams comparing liquid biopsy compartments, this is one reason exosomal proteins are attractive liquid biopsy targets: improved cargo stability and persistent biological signal.
Why "multi-protein signatures" beat single markers in heterogeneous cancers
The most consequential shift in current biomarker discovery is not about which protein is best—it's about abandoning the idea that one protein can carry a cancer diagnosis, subtype classification, and prognosis across heterogeneous patients.
Single-marker discovery is fragile in preclinical cohorts because many proteins are not tumor-exclusive. Acute-phase responses, systemic inflammation, and tissue injury can all elevate proteins that look "cancer-associated" in small datasets. That is why single markers are vulnerable to false positives in conditions that co-occur with cancer (for example, pancreatitis in PDAC research).
Multi-protein exosomal panels change the statistical game:
- They capture complementary biology (tumor cell state, stromal remodeling, immune interaction).
- They enable classifier-based predictive power (logistic regression, random forests, regularized models) rather than a single cutoff.
- They are more robust to confounders because no single feature needs to remain perfectly specific.
For MOFU-stage readers—PIs, translational directors, and core managers—the practical implication is clear: treat exosomal proteomics as a platform for signature discovery and verification, not as a search for a single universal antigen.
Key Takeaway: In early-stage models, the limiting factor is often detectability, not algorithm choice. Exosomal proteins win because the biology yields more stable, earlier signal—and multi-protein signatures reduce false positives in noisy cohorts.
Pancreatic Cancer: Surface Biomarkers for Early-Stage Liquid Biopsy Research
PDAC remains a high-priority target for liquid biopsy innovation because it is often diagnosed late, progresses aggressively, and has few reliable early-stage screening markers. Even in well-controlled research cohorts, investigators face the same uncomfortable reality: the earlier the tumor, the harder it is to detect with conventional circulating analytes.
Exosomal surface proteins are appealing in PDAC because they can be used for both biomarker readout and enrichment strategy—surface markers can guide immuno-capture workflows and simultaneously serve as classifier features.
Early-Stage Signatures and Glypican-1 (GPC1)
A milestone in PDAC exosome biomarker research was the report that Glypican-1 (GPC1)—a heavily glycosylated cell-surface proteoglycan—was enriched on cancer cell-derived exosomes and could distinguish early PDAC from healthy controls in research cohorts. The biological logic is compelling: a tumor-associated surface protein displayed on vesicles that are continually released into blood can, in principle, provide a sensitive readout at low tumor burden.
In translational practice, GPC1 is best interpreted as a panel component and an enrichment handle, not as a standalone determinant. The reasons are methodological, not ideological:
- Exosome isolation method (ultracentrifugation vs SEC vs immunoaffinity) can shift apparent abundance.
- Antibody performance matters for surface-marker assays.
- Cohort composition (inflammatory controls, benign lesions) strongly affects specificity.
The research opportunity is not simply to re-test GPC1, but to determine the contexts in which it generalizes and how it performs alongside other vesicle-associated markers.
Benchmarking and Multi-Marker Integration
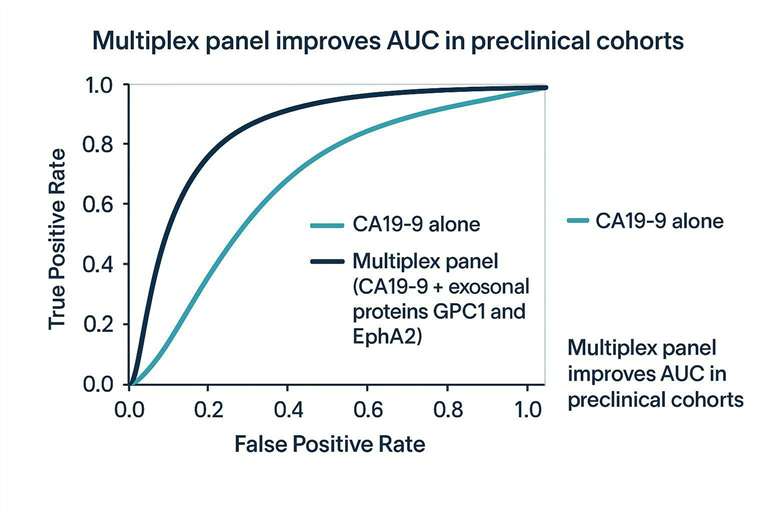
A common translational strategy is to benchmark novel exosomal membrane proteins alongside existing standards such as CA19-9. In PDAC, soluble CA19-9 is widely used in research and clinical monitoring, yet it is not sufficiently specific for early detection, and it can be elevated in benign inflammatory conditions.
Integrating EV proteomics with conventional markers can improve ROC performance in preclinical cohorts by:
- capturing tumor-associated surfaceome features (e.g., GPC1)
- adding orthogonal vesicle markers (e.g., EphA2, CD44v6, TSPAN8)
- reducing background noise from pancreatitis-like inflammation by requiring multi-feature concordance
A useful way to think about the "lift" is mechanistic: CA19-9 reflects one axis of disease-associated glycan biology, while exosomal panels can sample multiple axes—tumor cell state, invasion programs, stromal signals, and immune interaction.
The table below summarizes why combined strategies may provide stronger performance than single measurements in heterogeneous PDAC cohorts.
| Strategy | What it captures well | Typical failure mode in PDAC cohorts | Best use in preclinical workflows |
|---|---|---|---|
| CA19-9 alone | A known soluble marker with established assays | Elevated in benign inflammation; limited early-stage sensitivity | Baseline comparator; longitudinal monitoring feature |
| Single exosomal surface marker (e.g., GPC1) | Tumor-associated vesicle display | Isolation/assay bias; cohort-specific specificity | Enrichment handle; one feature within a classifier |
| Multi-protein exosomal panel | Complementary tumor + microenvironment signals | Overfitting in small discovery cohorts | Discovery → verification pipeline; classifier development |
| Combined CA19-9 + exosomal panel | Orthogonal biology + robustness | Requires careful calibration and QC | Highest-value approach for translational evaluation |
A practical note for program design: if your goal is to discover and verify a PDAC signature, upstream sample quality and vesicle purity will dominate downstream statistics. In that workflow context, teams often pair discovery LC-MS/MS with standardized isolation/characterization steps; when outsourcing or scaling, it can be useful to reference established EV pipelines such as Exosome Isolation and Purification Service and Exosomes Identification Service as examples of how isolation and verification steps can be modularized.
Lung Cancer: Stratifying Subtypes and Exploring Immune Evasion
Lung cancer liquid biopsy research has two persistent hurdles: (1) heterogeneity across histologies and molecular subtypes (NSCLC vs SCLC, driver-positive vs driver-negative), and (2) the need to distinguish malignant nodules from benign inflammatory lesions at the molecular level.
Exosomal proteomics is attractive here because it supports both subtype-linked signatures and immune phenotype readouts—the latter being critical for understanding and predicting response or resistance to immune checkpoint inhibitors.
Predictive Panels and Immune Checkpoint Markers
Preclinical and translational studies have reported exosomal protein signatures associated with NSCLC progression and tumor biology, including proteins linked to extracellular matrix remodeling, immune modulation, and oncogenic signaling. Examples often discussed in the literature include antigenic proteins (e.g., NY-ESO-1) and pathway-linked cargo reflecting EGFR alterations or downstream signaling states.
However, one exosomal protein has become a focal point because it links immune-evasion mechanisms with biomarker potential: exosomal PD-L1.
Tumor cells can package PD-L1 onto exosomes, effectively distributing an immune-inhibitory ligand systemically. In functional terms, exosomal PD-L1 can suppress circulating CD8+ T cell activity beyond the local tumor microenvironment. For translational researchers, this is valuable in two ways:
- Mechanism-of-action (MoA) insight: exosomal PD-L1 provides a measurable readout of immune-evasion strategy.
- Biomarker hypothesis: dynamic exosomal PD-L1 levels may correlate with immunotherapy response or resistance patterns, particularly when tissue PD-L1 is an imperfect surrogate for evolving systemic immune modulation.
This does not mean exosomal PD-L1 is "ready" as a clinical diagnostic. It does mean it is an unusually coherent target for integrated studies: discovery proteomics to identify co-traveling immune signals, targeted quantification to track dynamics, and functional assays to test immunosuppression.
In practice, the most informative experimental designs treat exosomal PD-L1 as part of a broader immune checkpoint and inflammation-aware panel—because immune state is multivariate. If you are designing an EV proteomics discovery-to-verification workflow in lung cancer, a useful reference point for the scope of typical EV proteomics pipelines is Extracellular Vesicles Proteomics Services.
Breast Cancer: Subtyping and the Pre-Metastatic Niche
Breast cancer liquid biopsy research is not limited to early detection. In many programs—especially those focused on aggressive molecular subtypes like triple-negative breast cancer (TNBC)—the more strategic goal is understanding metastatic risk, monitoring treatment response, and identifying mechanisms that enable organ-specific colonization.
Exosomes are central to this research direction because they are not merely passive biomarkers; they participate in remodeling distant tissues. That makes exosomal proteins particularly informative: they can report on (and contribute to) the metastatic program.
Organotropic Metastasis and Integrin Signatures
One of the most influential concepts in metastasis biology is the "pre-metastatic niche"—the idea that primary tumors can condition distant organs before tumor cells arrive. Tumor-derived exosomes are now understood as one vehicle for that conditioning.
A landmark mechanistic finding is that specific exosomal integrin signatures can bias organotropism:
- exosomal integrins α6β4 and α6β1 have been linked to lung-tropic behavior
- exosomal integrin αvβ5 has been linked to liver-tropic behavior
For translational teams, this matters because it reframes what an "exosomal biomarker" can be. Instead of only asking whether a protein distinguishes cancer vs non-cancer, you can ask whether a protein panel predicts trajectory—which patients or models are on a lung-metastatic vs liver-metastatic path, and what upstream pathways might be druggable.
Methodologically, these integrin-focused signatures also highlight why deep, unbiased proteomics is often necessary at discovery stage: integrin family members and their co-factors can be difficult to capture with antibody-only strategies, and their interpretation benefits from pathway-level context.
Bridging the Translational Gap: From Discovery to Large-Cohort Verification
Discovery proteomics can generate long lists of candidate proteins from tumor models or small patient sets. The hard part is what comes next: determining which candidates remain significant when you scale from dozens of samples to hundreds, across different sites, operators, instruments, and pre-analytic variables.
This "verification gap" is where many EV biomarker programs stall—not because the biology is uninteresting, but because the data can be brittle.
Overcoming Overfitting in Preclinical Cohorts
Overfitting is the default risk in small discovery cohorts, especially when the feature space is large (hundreds to thousands of proteins) and the number of samples is modest. EV proteomics adds extra degrees of freedom: isolation method, storage, hemolysis, lipoprotein contamination, and digestion efficiency can all imprint technical structure onto the dataset.
To reduce overfitting risk, preclinical and translational teams typically adopt a verification mindset early:
- Lock your candidate list before looking at the validation cohort.
- Use independent cohorts (ideally multi-center) to test generalizability.
- Add orthogonal measurements when feasible (e.g., targeted MS plus an antibody-based assay for a subset), not to "prove" the biology but to detect method-specific artifacts.
- Document pre-analytics and QC as first-class variables, not footnotes.
Pro Tip: If a signature's AUC collapses when you swap isolation method—or when you introduce inflammatory controls—it may still be biologically real. The failure is that the signature is not robust enough for your intended use case.
Targeted PRM Mass Spectrometry for Biomarker Verification
Parallel Reaction Monitoring (PRM) mass spectrometry is widely used as an analytical bridge between unbiased discovery and large-cohort verification because it can quantify multiple proteins with high specificity without requiring new antibodies for each target.
In EV biomarker programs, PRM is especially valuable because many of the most interesting candidates are:
- novel or poorly characterized
- membrane-associated or highly modified
- difficult to assay by ELISA due to antibody availability and epitope constraints
A PRM verification workflow typically supports:
- multiplex quantification of dozens of candidate proteins in one run
- consistent peptide-level specificity for proteins with close homologs
- scalability to large translational cohorts when sample prep is standardized
From a study-design standpoint, PRM also forces a healthy discipline: you must define target peptides, transitions, and QC rules upfront. That makes the verification stage less vulnerable to "researcher degrees of freedom" that inflate discovery performance.
Supporting Discovery-to-Verification EV Proteomics Workflows
Advancing exosomal protein signatures in PDAC, lung cancer, and breast cancer typically requires two complementary capabilities: deep unbiased LC–MS/MS discovery to identify candidate panels, and targeted verification to evaluate those panels across larger cohorts.
Researchers developing end-to-end EV biomarker workflows may benefit from service pipelines that combine EV-specific sample handling, discovery proteomics, and targeted verification, such as Exosome Proteomics Services and Extracellular Vesicles Proteomics Services.
Frequently Asked Questions
Why measure multi-protein signatures in exosomes rather than single soluble proteins in plasma?
Multi-protein signatures in exosomes are typically more robust because exosomes enrich and protect low-abundance, tumor-associated proteins while reducing exposure to plasma's highly abundant acute-phase proteins. A panel also captures complementary biology (tumor state, immune interaction, microenvironment remodeling), which reduces false positives driven by inflammation or sample-to-sample variability.
Are these exosomal protein biomarkers intended for immediate clinical diagnosis?
No. In most studies, these candidates are positioned as Research Use Only (RUO) markers for discovery and translational verification, not as stand-alone clinical diagnostics. The near-term research priority is to standardize workflows and verify signatures across independent cohorts so performance reflects biology rather than cohort-specific artifacts.
Can mass spectrometry accurately detect low-abundance targets like PD-L1 on exosomes?
Yes—when EV isolation, lysis/digestion, and peptide selection are explicitly optimized for membrane proteins and low-input samples. Targeted MS approaches (including PRM) can quantify low-abundance targets with peptide-level specificity, but sensitivity depends heavily on upstream EV purity, losses during prep, and rigorous QC.
What is an exosome liquid biopsy, and how is it different from ctDNA-based liquid biopsy?
An exosome liquid biopsy analyzes tumor-associated extracellular vesicles—often focusing on their protein, RNA, or lipid cargo—while ctDNA assays detect tumor-derived DNA fragments. In early-stage models, exosomes can offer earlier and more stable access to tumor-associated biology because vesicles are actively shed and their cargo is protected in biofluids.
Can exosome liquid biopsy detect early-stage pancreatic cancer in research settings?
In research cohorts, early-stage signal is often more detectable in EV-associated cargo than in ctDNA or CTCs, but performance depends on study design, controls (including pancreatitis), and method standardization. The most reliable approach is usually not a single marker but a multi-protein classifier that is verified in independent cohorts.
Are exosomal integrins really predictive of where breast cancer will metastasize?
Exosomal integrin patterns have been reported to influence and reflect organotropic metastasis biology, particularly in mechanistic studies of the pre-metastatic niche. For translational use, integrin features should be treated as hypothesis-generating components of broader signatures and verified across cohorts and platforms before being used as predictive markers.
What is PRM mass spectrometry and why is it used for biomarker verification?
PRM (Parallel Reaction Monitoring) is a targeted mass spectrometry method that quantifies predefined peptides with high specificity and multiplexing capacity. It's used for verification because it can measure many candidate proteins simultaneously without requiring new antibodies, making it well-suited for scaling signature testing across large cohorts.
References
- Glypican-1 identifies cancer exosomes and detects early pancreatic cancer
- Exosomal PD-L1 contributes to immunosuppression and is associated with anti-PD-1 response in melanoma
- Suppression of Exosomal PD-L1 Induces Systemic Anti-tumor Immunity and Memory
- Exosomal integrins dictate organotropic metastasis
* For Research Use Only. Not for use in diagnostic procedures.
